



























Scoliosis

What is scoliosis?
Scoliosis is a sideways curvature of the spine. The spine naturally has slight forward and backward curves. But in scoliosis, the spine curves to the left or right in a C shape or both ways in an S shape. The curve has to be greater than 10 degrees as measured on X-ray to be considered scoliosis. Anything less than 10 degrees is considered a normal variation.Types of scoliosis
Scoliosis may be divided into five principal types:
- Idiopathic scoliosis. This is the most common form of scoliosis. The term idiopathic means the cause is unknown. Affected children are otherwise healthy. Though the spine curves, the vertebrae show no abnormality on X-rays or when observed directly in the operating room. While the overall incidence is equal in girls and boys, idiopathic scoliosis that is progressive or severe is about six to seven times more common in girls than in boys.
- Congenital scoliosis. This type of scoliosis occurs because the spine didn't develop properly while the baby was in utero. The problem usually isn't apparent until childhood or adolescence.
- Neuromuscular scoliosis. This is scoliosis caused by a disorder, such as spina bifida or cerebral palsy, or a spinal cord injury, all of which can damage nerves and muscles so that they don't support the spine properly.
- Syndromic scoliosis. Scoliosis can be one of the issues associated with certain conditions, such as Marfan syndrome, muscular dystrophy or Ehlers-Danlos syndrome.
- Postural scoliosis. This type of scoliosis may be a response to pain, as the child tilts sideways to alleviate discomfort. It can be reversed by relieving the pain or by having the child lie flat. X-rays don't show any abnormality of the vertebrae.
Symptoms of scoliosis
Symptoms vary depending on the degree of spinal curvature. Visible signs include:
- Uneven shoulders.
- Uneven waist.
- One shoulder blade is more prominent or visible than the other.
- One hip appears higher than the other.
- One leg appears shorter than the other.
- The ribs stick out farther on one side of the body.
- One side of the rib cage is higher than the other when the patient bends forward.
- The head isn't centered above the pelvis.
- Loss of height.
- Misalignment in pelvis and hips.
The condition can also cause:
- Back pain and stiffness
- Leg pain, numbness or weakness
- Trouble standing up straight
- Weak core muscles
If you notice any of these signs, schedule a checkup with your child's health care provider.
Signs and complications of progressive scoliosis
Progressive scoliosis is when the curvature worsens over time. This can lead to additional problems, including:
- Breathing difficulties
- Heart problems
- Back pain
- Changes in posture
- Self-consciousness or esteem issues, as the curvature becomes visible to others
Diagnosis of scoliosis
A school nurse, pediatrician or orthopedic surgeon will perform a physical exam in order to make this diagnosis. The main sign is asymmetry of the shoulders or torso or one side of the rib cage being higher when the child bends forward. Other signs of scoliosis include tilting of the pelvis – which may make one leg appear shorter than the other – and a difference in the contours of the sides of the body between ribs and hips.
In addition to checking for these differences, the doctor may order X-rays to see the alignment of the vertebrae. These images can be used to determine the degree of spinal curvature and to help monitor its progression over time.
Certain types of scoliosis are associated with other conditions. If a child with scoliosis is suspected of having an underlying disease, more tests may be necessary, including:
- Ultrasound. This imaging test uses sound waves to detect abnormalities in soft tissue and organs.
- Magnetic resonance imaging (MRI). The detailed images provided by this scan can reveal abnormalities that may be contributing to scoliosis, such as malformations or tumors in the spinal cord, nerves and other structures.
Treatment of scoliosis
The younger a child when diagnosed, or the more time they have left to grow, the greater the risk of scoliosis progressing. After puberty, curves less than 50 degrees are unlikely to get worse. For this reason, the ultimate goal of scoliosis management is to keep curves at less than 50 degrees until your child has matured. Children with these lesser curves typically grow into adults with no significant problems related to scoliosis.
Scoliosis treatment options depend on the degree of curvature of the spine, viewed from the front or back by X-ray. The following are general guidelines for treatment.
Less than 10 degrees of spinal curvature
This is not scoliosis. Scoliosis is defined as spinal curvature greater than 10 degrees. Anything under 10 degrees is considered a normal variation, just as there are normal ranges for weight and height.
10 to 30 degrees of spinal curvature
In this range, scoliosis is monitored for progression. The measurement error in reading X-rays is up to 4 degrees. This means that a difference of 4 degrees between office visits may not be real but rather a reflection of the inherent inaccuracies of measuring X-rays. Partly because of this, significant progression is defined as an increase in curvature of at least 5 degrees.
The typical rate of progression is 1 degree per month, so it would take at least five months to see significant progression. As a result, children should be seen every six months for follow-up, having both a physical exam and X-rays.
30 to 50 degrees of spinal curvature
In this range, bracing is the standard of care in the United States. The scoliosis brace is known as a thoracolumbar sacral orthosis (TLSO). The idea behind bracing is to stop or slow curve progression so that it stays under 50 degrees.
The brace is worn more than 20 hours per day. Time out of the brace is allowed for bathing and sports. Part-time bracing doesn't work as well – and may not work at all.
Your child will be fitted for a custom-made brace and gradually transitioned to wearing it full-time over a two-week period. This allows your child time to adjust and prevents significant skin irritation from the brace. Brace treatment continues until the child is finished growing and the spine has reached its adult length.
Successful bracing reduces the curve by 50% or more, as determined by X-rays. At later visits, X-rays are taken of the child out of the brace, which is removed the night before to allow full relaxation of the spine and a more realistic measure of the remaining degree of curvature. Brace treatment stops curve progression in about 80% of children.
More than 50 degrees of spinal curvature
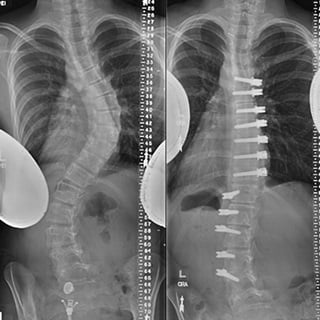
Beyond 50 degrees, the spine loses its ability to compensate, and progression becomes inevitable even after physical maturity. The only way to stop progression at this stage is through surgery, either spinal fusion or vertebral body tethering. In spinal fusion surgery, metal implants are used to realign and fuse the vertebrae in a way that corrects the curve.
Vertebral body tethering
Doctors at UCSF were at the forefront of testing vertebral body tethering (VBT), a cutting-edge treatment for children with scoliosis. VBT is a surgical procedure that uses a flexible cord to straighten the spine and guide its growth while maintaining flexibility and motion. Unlike traditional methods, such as bracing or spinal fusion, VBT corrects the spinal curve and allows your child to stay active.
This treatment is ideal for children with a spine curvature of 40 to 70 degrees and bones strong enough to withstand the tether. VBT is also typically most effective for children between 10 and 14 because it relies on the continued growth of the spine.
There's no clear evidence that scoliosis – treated or untreated – will increase the risk of back pain or arthritis later in life.
More treatment info
-

Spinal fusion surgery
Our pediatric orthopedic surgeons perform spinal fusion surgery, which corrects severe scoliosis by connecting spinal bones.
Learn more -
Vertebral body tethering
This surgery for scoliosis uses your child's own growth to straighten the spine and may offer advantages over traditional approaches.
Learn more
UCSF Benioff Children's Hospitals medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your child's doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your child's provider.
Where to get care (7)
Clinical trials
See all clinical trials
0 in progress, 1 open to new patients
The Effect of Erector Spinae Plane Block (ESPB) on Pediatric Pain Management Following Posterio...
Institutional pain management protocol: patients have a hydromorphone patient-controlled analgesia pump until post-operative day 1 and as needed (PO) methadone two times a day, as well as PO oxycodone every 4 hours as needed for m...
Recruiting
More about this studyAwards & recognition
-

One of the nation's best for orthopedics
-

Ranked among the nation's best in 11 specialties