













Smell the roses
Wander outside into our Butterfly Garden in Oakland and our healing gardens at Mission Bay.




Here to serve you
Explore our network of care for kids, from the tiniest to teens and young adults.




World-class docs
We'll help you find the best provider for your child.




Stress-free visits
Accommodations. Admission. Discharge. Procedure prep. We've got you covered.




Extraordinary kid care
Our specialists handle conditions ranging from the common to the most rare.




Referrals made easy
Contacts and resources to get your patients to our pediatric specialists




Best in Northern CA
We're ranked #1 in pediatric cancer, heart surgery, cardiology & more.





A craniopharyngioma is a type of brain tumor that occurs under and behind the brain's frontal lobes. The tumor begins from a remnant of tissue adjacent to the pituitary, a gland that regulates many hormones and is connected to a part of the brain called the hypothalamus. The optic nerves, which connect the eyes to the brain, meet directly above the pituitary gland.
Craniopharyngiomas are considered benign (not cancerous) tumors. If the tumor is removed completely, or partially removed and treated effectively with radiation, the long-term outcome is quite good for most patients. But for some patients, the tumor will return despite many therapies. In general, older children with smaller tumors fare better than young children, or children of any age with very large tumors.
Because of their location, craniopharyngiomas cause symptoms by affecting the important adjacent structures such as the pituitary gland, hypothalamus and optic nerves.
Symptoms, which depend on the patient's age, may include:
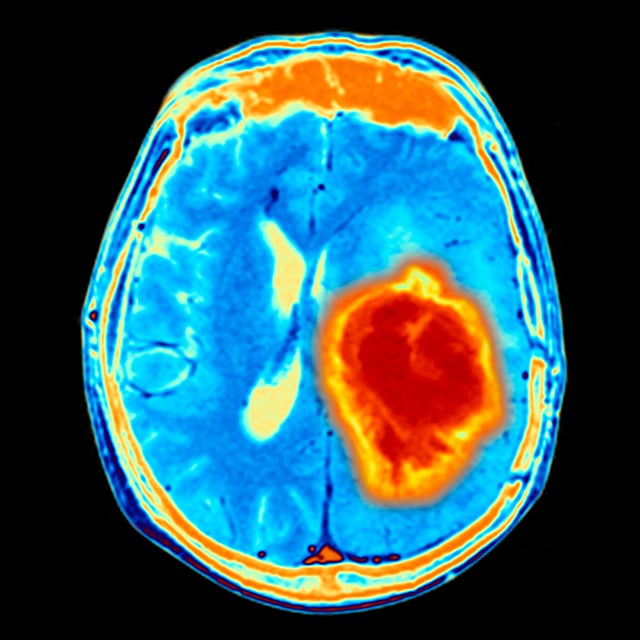
Most patients are diagnosed with a craniopharyngioma when symptoms — such as vision disturbance, hormonal problems or headaches related to hydrocephalus — lead to an imaging study such as an MRI scan. The scan usually shows the characteristic features of the tumor — its location directly next to the pituitary gland, as well as other features such as calcification and cysts — making the diagnosis fairly straightforward.
Treatment often requires surgery and sometimes radiation therapy. Depending on the severity of the symptoms at the time of diagnosis, patients can make a complete recovery. However, because craniopharyngiomas can involve important structures in the brain, tumor growth or treatments can cause permanent problems, such as lack of normal hormone control, vision loss or the need for a shunt to treat hydrocephalus.
In general, most children with craniopharyngiomas will require long-term monitoring and treatment of endocrine function (and treatment if the pituitary is not functioning properly), as well as regular MRI scans to check for any signs that the tumor has returned.
Choosing a treatment is often a challenge. The goals of a cure or good tumor control must be balanced against unacceptable side effects from the treatment.
If the tumor is not tightly attached to important brain structures, and can be removed completely by surgery, a cure is possible. This occurs in about a third of cases.
In the majority of the remaining cases, the tumor can be mostly removed, leaving a small amount behind. In general, if there is doubt about whether any part of the tumor is left after surgery, radiation is recommended to prevent recurrence of the tumor. The type of radiation used depends on the location of the residual tumor.
If a larger amount of tumor remains after surgery, or if vital structures are close by, then conformal external beam radiotherapy is used. This method uses many smaller doses of radiation to protect the surrounding brain tissue, but there is some spread of the radiation beyond the actual target. Nevertheless, this technique is very safe and has excellent results.
If there is a small, well-defined residual tumor remaining that is a safe distance from the optic nerves and hypothalamus, Gamma Knife radiosurgery is an option. However, radiation usually affects the pituitary function and can affect cognitive function. For young children who have had a good surgical resection (removal of most of the tumor), an alternative option is the "watch and wait" approach, with radiation treatment given only if there is clear evidence of recurrent tumor growth.
UCSF Benioff Children's Hospitals medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your child's doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your child's provider.

One of the nation's best for neurology & neurosurgery

Ranked among the nation's best in 11 specialties
Smell the roses